
Wywieranie presji przez przemysł zakłócające badania, strategie, nakłady i praktyki w zakresie ochrony zdrowia: przegląd
Emmanuel Stamatakis*, Richard Weiler i John P.A. Ioannidis
Abstrakt
Tło: Nakłady na produkty przemysłowe (w większości leki i wyroby medyczne) w ciągu ostatnich 15 lat rosły lawinowo i obejmują obecnie znaczną część nakładów na opiekę zdrowotną. Ogromne udziały finansowe włożone w opracowanie i marketing leków i wyrobów medycznych mogły wywoływać nadmierną presję na przemysł farmakologiczny by wpływać na badania medyczne oraz politykę i praktykę w zakresie zdrowia.
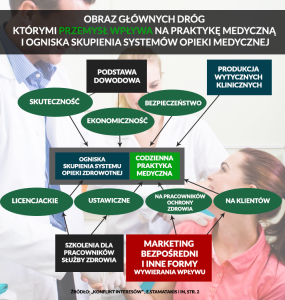
Materiały i metody: Przegląd literatury oraz analiza różnych dróg, którymi przemysł farmakologiczny bezpośrednio lub pośrednio przenika do szerzej rozumianego systemu opieki zdrowotnej. Przedstawiamy analizę wpływu przemysłu na następujących poziomach: (i) produkcja podstaw dowodowych, (ii) synteza dowodów, (iii) rozumienie kwestii bezpieczeństwa i szkodliwości, (iv) ocena kosztów, (v) tworzenie wytycznych dla praktyki klinicznej, (vi) szkolenia dla pracowników służby zdrowia, (vii) praktyka medyczna, (viii) decyzje klientów opieki zdrowotnej.
Wyniki: Przedstawiliśmy wiele spójnych dowodów wykazujących fakt utworzenia przez przemysł środków interwencji na wszystkich etapach procesów decydujących w zakresie badań medycznych, strategii, nakładów, praktyki i edukacji w zakresie ochrony zdrowia. W wyniku tych ingerencji, korzyści stosowania leków i innych produktów często są wyolbrzymiane w stosunku do możliwej szkodliwości, którą się bagatelizuje, a wytyczne kliniczne, praktyka medyczna i nakłady na opiekę zdrowotną są realizowane w oparciu o stronnicze decyzje.
Wniosek By móc służyć swoim interesom, przemysł medyczny mistrzowsko wpływa na produkcję podstaw dowodowych, syntezę dowodów, rozumienie kwestii szkodliwości, szacunek kosztów, wytyczne kliniczne i szkolenia dla pracowników służby zdrowia, jak również wywiera bezpośredni wpływ na decyzje podejmowane przez pracowników i klientów opieki zdrowotnej. Istnieje pilna potrzeba podejmowania działań regulacyjnych i innych mających na celu ponowne zdefiniowanie misji medycyny tak by była bardziej ukierunkowana na dobro pacjenta, populacji i społeczeństwa, czyli by była wolna od konfliktu interesów.
Eur J Clin Invest 2013; 43 (5): 469?475
Referencje:
- The Lancet (in-house editorial). Lessons from Lipitor and the broken blockbuster drug model. Lancet2011;378:1976.
- 2International Monetary Fund. World Economic Outlook Database [Internet]. Nominal GDP list of countries for the year 2010. 2011. Available at: www.imf.org/external/pubs/ft/weo/2011/02/weodata/index.aspx. updated on 24 January 2012.
- 3, . The need to consider the wider agenda in systematic reviews and meta-analyses: breadth, timing and depth of evidence. BMJ 2010;341:c4875. doi:10.1136/bmj.c4875.
- 4Abbott. 2009 Annual Report [Internet] 2009. Available at: http://www.abbott.com/annual-reports/2009/downloads/Editorial_section_only.pdf. cited on 12 February 2013.
- 5MassDevice staff. MassDevice Blog: Abbott Labs and Boston Scientific together make up about 64 percent of U.S. drug eluting stent market [Internet]. c2011. Available at: http://www.massdevice.com/news/abbott-and-boston-scientific-dominate-46-billion-drug-eluting-stent-market. cited on 12 February 2013.
- 6, , . Reversals of established medical practices: evidence to abandon ship. JAMA2012;307:37?8.
- 7, . Percutaneous coronary intervention versus conservative therapy in nonacute coronary artery disease. Circulation 2005;111:2906?12.
- 8, , , , , et al. Optimal medical therapy with or without PCI for stable coronary disease. N Engl J Med 2007;356:1503?16.
- 9, . Initial coronary stent implantation with medical therapy vs medical therapy alone for stable coronary artery disease: meta-analysis of randomized controlled trials. Arch Intern Med2012;172:312?9.
- 10, , , . Pharmaceutical industry sponsorship and research outcome and quality: systematic review. BMJ 2003;326:1167?70.
- 11, , , . Association of funding and conclusions in randomized drug trials: a reflection of treatment effect or adverse events? JAMA 2003;290:921?8.
- 12, , , . Industry sponsorship and selection of comparators in randomized clinical trials. Eur J Clin Invest 2010;40:172?82.
- 13, , , . Outcome reporting in industry-sponsored trials of gabapentin for off-label use. N Engl J Med 2009;361:1963?71.
- 14, , , . Guest authorship and ghostwriting in publications related to rofecoxib: a case study of industry documents from rofecoxib litigation. JAMA 2008;299:1800?12.
- 15. Ghosts in the Machine. Soc Stud Sci 2009;39:171?98.
- 16, , , . Conflicts of interest at medical journals: the influence of industry-supported randomised trials on journal impact factors and revenue ? cohort study.PLoS Med 2010;7:e1000354.
- 17. Meta-research: the art of getting it wrong. Res Synth Methods 2010;1:169?84.
- 18, , . Rethinking credible evidence synthesis. BMJ 2012;344:d7898.
- 19, , . Cochrane reviews compared with industry supported meta-analyses and other meta-analyses of the same drugs: systematic review. BMJ 2006;333:782.
- 20, , . Financial ties and concordance between results and conclusions in meta-analyses: retrospective cohort study. BMJ 2007;335:1202?5.
- 21, , , , , et al. Reporting of conflicts of interest in meta-analyses of trials of pharmacological treatments. JAMA 2011;305:1008?17.
- 22, . Content area experts as authors: helpful or harmful for systematic reviews and meta-analyses? BMJ 2012;345:e7031.
- 23, , , , , . Timing of new black box warnings and withdrawals for prescription medications. JAMA 2002;287:2215?20.
- 24. Rosiglitazone: what went wrong? BMJ 2010;341:c4848.
- 25, , , . Association between industry affiliation and position on cardiovascular risk with rosiglitazone: cross sectional systematic review. BMJ 2010;340:c1344.
- 26, , , , , et al. The adenomatous polyp prevention on Vioxx trial investigators. Cardiovascular events associated with rofecoxib in a colorectal adenoma chemoprevention trial. N Engl J Med 2005;352:1092?102.
- 27, , . Expression of concern: Bombardier et al., ?Comparison of upper gastrointestinal toxicity of rofecoxib and naproxen in patients with rheumatoid arthritis?. N Engl J Med2000;343:1520?8. N Engl J Med 2005;353:2813?4.
- 28. For Merck, Vioxx paper trail won’t go away. New York Times. 2005 Aug 21; Sect A:1.
- 29, , , , , et al. Bias in published cost effectiveness studies: systematic review. BMJ 2006;332:699?703.
- 30, , , . Comparing estimates of cost effectiveness submitted to the National Institute for Clinical Excellence (NICE) by different organisations: retrospective study. BMJ2005;330:65.
- 31, , , . Industry involvement and baseline assumptions of cost-effectiveness analyses: diagnostic accuracy of the Papanicolaou test. CMAJ 2011;183:E337?43.
- 32, , , . Huge impact of assumptions on indirect effects on the cost-effectiveness of routine infant vaccination with 7-valent conjugate vaccine (Prevnar). Vaccine2010;28:2367?9.
- 33, , , , . Conflicts of interest in cardiovascular clinical practice guidelines. Arch Intern Med 2011;171:577?84.
- 34, , , . Prevalence of financial conflicts of interest among panel members producing clinical practice guidelines in Canada and United States: cross sectional study. BMJ2011;343:d5621.
- 35, , , . Conflict of interest in clinical practice guideline development: a systematic review. PLoS One 2011;6:e25153.
- 36, , , , . Scientific evidence underlying the ACC/AHA clinical practice guidelines. JAMA 2009;301:831?41.
- 37, , . Relationships between authors of clinical practice guidelines and the pharmaceutical industry. JAMA 2002;287:612?7.
- 38, . Glycemic control in type 2 diabetes: time for an evidence-based about-face? Ann Intern Med 2009;150:803?8.
- 39, , . Intensified glucose lowering in type 2 diabetes: time for a reappraisal.Diabetologia 2010;53:2079?85.
- 40, , , , , . Failure to discount for conflict of interest when evaluating medical literature: a randomised trial of physicians. J Med Ethics2010;36:265?70.
- 41. Key opinion leaders: independent experts or drug representatives in disguise? BMJ2008;336:1402?3.
- 42. Key opinion leaders: where they come from and how that affects the drugs you prescribe.Dermatol Ther 2009;22:262?8.
- 43, , , , , et al. Clinical equivalence of generic and brand-name drugs used in cardiovascular disease: a systematic review and meta-analysis.JAMA 2008;300:2514?26.
- 44, , , , , et al. Medical students’ exposure to and attitudes about drug company interactions. JAMA 2005;294:1034?42.
- 45, , . Medical students’ exposure to and attitudes about the pharmaceutical industry: a systematic review. PLoS Med 2011;8:e1001037.
- 46, , , . Effect of exposure to small pharmaceutical promotional items on treatment preferences. Arch Intern Med 2009;169:887?93.
- 47, , , , , et al. Institutional academic industry relationships. JAMA 2007;298:1779?86.
- 48, , . Industry support of CME ? are we at the tipping point? N Engl J Med2012;366:1069?71.
- 49, . Funding for medical education: maintaining a healthy separation from industry.Circulation 2010;121:2228?34.
- 50. Physicians and the pharmaceutical industry: is a gift ever just a gift? JAMA 2000;283:373?80.
- 51. Pharmaceutical Industry financial support for medical education; benefit, or undue harm? J Law Med Ethics 2009;37:451?60.
- 52, , , , , . A national survey of physician-industry relationships. N Engl J Med 2007;356:1742?50.
- 53, . The cost of pushing pills: a new estimate of pharmaceutical promotion expenditures in the United States. PLoS Med 2008;5:e1.
- 54, . Physicians’ behavior and their interactions with drug companies: a controlled study of physicians who requested additions to a hospital drug formulary. JAMA 1994;271:684?9.
- 55, . Arabian nights?1001 tales of how pharmaceutical companies cater to the material needs of doctors: case report. BMJ 2000;321:1563?4.
- 56, . Norgine’s reply to ABPI. BMJ 2010;340:c1869.
- 57, , , . The impact of disclosing financial ties in research and clinical care: a systematic review. Arch Intern Med 2010;170:675?82.
- 58, , , . Costs and consequences of direct-to-consumer advertising for clopidogrel in Medicaid. Arch Intern Med 2009;169:1969?74.
- 59, , . A decade of direct-to-consumer advertising of prescription drugs.N Engl J Med 2007;357:673?81.
- 60Kaiser Family Foundation [Internet]. Prescription Drug Trends. Menlo Park, California; c2010. Available at:http://www.kff.org/rxdrugs/upload/3057-08.pdf. cited on 12 February 2013.
- 61. Drug risks and free speech: can congress ban consumer drug ads? N Engl J Med2007;356:2236?9.
- 62Institute of Medicine. Chapters 3?8. In: Lo B, Fields MJ, editors. Conflict of Interest in Medical Research, Education, and Practice. Washington, DC: National Academy of Sciences; 2009: pp. 62?229.